
From the 1Department of Orthopaedic Surgery and 2Section of Sport Science, Department of Public Health, Aarhus University, Denmark, 3Department of Physiotherapy, Faculty of Health Sciences, VIA University College, Aarhus, 4Department of Orthopaedic Surgery, Horsens Hospital, Horsens, 5Centre of Research in Rehabilitation (CORIR), Department of Clinical Medicine, Aarhus University Hospital and Aarhus University, Aarhus, Denmark
Objectives: To examine whether progressive resistance training is feasible in patients with symptomatic hip dysplasia scheduled for periacetabular osteotomy. A secondary objective was to investigate patient-reported outcomes, functional performance and hip muscle strength.
Design: Feasibility study.
Patients and methods: Seventeen patients (median age 28 years, range 22–40 years) performed 8 weeks (20 sessions) of supervised sessions of progressive resistance training. Training-adherence, number of dropouts and adverse events, and visual analogue scale scores on pain were registered. Patients completed the Hip and Groin Outcome Score, performed 2 hop-tests, and hip peak torque was assessed by isokinetic dynamometry.
Results: Training-adherence was 90.3±9%. Few and minor adverse events were observed, one patient dropped out and acceptable pain levels were reported during the intervention. Scores on 4 out of 6 subscales on patient-reported outcome improved (p < 0.05), as did standing distance jump (12.2%, 95% confidence interval (CI) [1.3, 23.0]), countermovement jump (25.1%, 95% CI [1.3, 48.8]). Isokinetic concentric hip flexion peak torque showed significant improvements (16.6%, 95% CI [4.6, 28.6]) on the affected side while isometric hip flexion (10.9%, 95% CI [0.3, 21.6]) improved on the non-affected side.
Conclusion: Supervised progressive resistance training is feasible in patients with hip dysplasia. The intervention may improve pain levels, patient-reported outcomes, functional performance and hip flexion muscle strength.
Key words: hip; hip dysplasia; resistance training; strength; feasibility study.
Accepted May 28, 2018; Epub ahead of print Aug 8, 2018
J Rehabil Med 2018; 50: 751–758
Correspondence address: Louise Mortensen, Department of Orthopaedic Surgery, Aarhus University Hospital, Tage-Hansens Gade 2, DK-8000 Aarhus C, Denmark. E-mail: lpmortensen@hotmail.com
This study examined the feasibility of 8 weeks of progressive resistance training for patients with symptomatic hip dysplasia. Seventeen patients were included, and 16 completed the training intervention (20 sessions over 8 weeks). The study showed that patients with hip dysplasia were able to perform progressive resistance training with a substantial general load progression without increasing pain in the hip. Furthermore, the patients reported increased level of activities of daily living and function of the hip after the intervention. This study provides important knowledge on how patients with HD respond to resistance training.
Hip dysplasia (HD) is a well-known cause of hip pain and hip dysfunction (1, 2). Patients report decreased levels of activity, and HD is associated with an increased risk of developing secondary hip osteoarthritis (OA) (1, 3). The prevalence in the adult population of mild to moderate HD is 3.5% globally, and patients experience onset of symptoms during childhood (4). The preferred surgical treatment of symptomatic HD is the periacetabular osteotomy (PAO), which re-orientates the dysplastic acetabulum (5, 6). PAO seeks to correct abnormal biomechanics of the dysplastic hip, relieve symptoms to improve patient function and quality of life, and prevent or delay secondary OA (5, 7). Complications of the surgery may be expected in up to 15% of all cases (8) and at 4 to 12 years’ follow-up 13% of patients may still experience chronic pain and reduced physical function (9).
Despite the generally positive effects of exercise on muscle strength and physical function in hip OA (10–14) and in patients with groin pain (15, 16), exercise has only attracted little attention as a treatment to relieve symptomatic HD. Moreover, improving hip muscle strength preoperatively may be an effective way to optimize function and the outcome of PAO (17, 18). Also, an exercise intervention could potentially postpone or perhaps even replace a planned PAO, as seen in other related pathologies, such as knee OA (19). Nonetheless, no studies have investigated the use of a progressive resistance training (PRT) programme in patients with HD. Due to hip flexor and extensor deficits in patients with chronic hip pain (20–23) exercises should focus on increasing the strength of these muscle groups.
The aim of this study was to examine whether PRT is feasible in patients with symptomatic HD in terms of adherence, drop-outs, adverse events, eligibility and pain responses to the training intervention. A secondary purpose was to investigate data on changes in patient-reported outcome (PRO), functional performance and hip muscle strength after a PRT intervention. This information is important before initiating a large randomized controlled trial (RCT) investigating the effect of PRT in patients with symptomatic HD scheduled for PAO.
The present feasibility study was conducted at the Orthopaedic Department, Aarhus University Hospital, Denmark, and at the Section of Sports Science, Aarhus University, Denmark.
The study was conducted in accordance with the Declaration of Helsinki, and ethical approval was obtained from the Central Denmark Region Committee on Biomedical Research (journal number 1-10-72-236-15). Approval from The Danish Data Protection Agency (journal number 2007-58-0010) was obtained and all patients gave written informed consent prior to inclusion.
Inclusion criteria were: (i) diagnosis of HD, (ii) on waiting list for PAO surgery at Aarhus University Hospital, Denmark, (iii) living within 50 km of the training site, (iv) able to transport him- or her-self to the study location, and (v) age > 18 years. Exclusion criteria were: (i) Tönnis OA score > 1, (ii) retroverted acetabulum, (iii) other hip diseases, such as Calvé Perthes and epiphyseolysis, (iv) undergone surgery for a herniated disc and spondyloses, joint preserving or arthroplasty of the hip, knee, or ankle and arthroplasty of the knee or ankle on the affected side, (v) neurological or rheumatological diseases affecting hip function, (vi) tenotomy of the iliopsoas tendon or z-plastic of the iliotibial band, and (vii) body mass index ≥ 40 kg/m2.
The training protocol was designed in accordance with the guidelines of the American College of Sports Medicine (ACSM) for progression models in resistance training for healthy adults, and aims at increasing muscle strength and inducing muscle hypertrophy (24). A previous RCT by Skoffer et al. (25) showed that only 4 weeks of PRT is sufficient to increase muscle strength in patients with knee osteoarthritis. In this study all patients underwent 8 weeks of supervised PRT, with a total of 20 training sessions (5 sessions per 2 weeks). After a 5–10-min warm-up on a stationary bicycle, patients performed 5 different exercises for the lower extremities: leg press, hamstring curl, knee extension (all performed double-legged), hip flexion (performed single-legged) and lunges. Each session lasted approximately 45–60 min. Three to four sets of 8–12 repetitions were performed in all exercises, with the intensity increasing progressively from 12 repetitions (15 repetitions maximum (RM)) and 3 sets the first 2 weeks towards 8 repetitions (8 RM) and 4 sets in the last 2 weeks. The intensity was determined such that, if the patient was able to perform 2 or more repetitions than the target RM load in the last of the performed sets, then the load was increased. All sessions were supervised by a physiotherapist or by a sport science student to ensure sufficient loading and progression. Patients were asked not to receive any other form of treatment for the hip during the intervention period, and not to take any pain medication prior to a training session.
Feasibility and adherence. A 100-mm visual analogue scale (VAS) was used for pain assessment. Patients rated their pain levels during each exercise immediately after finishing the exercise. A mean pain score was calculated based on all scores obtained during the 5 individual exercises. At the following training session patients further reported their maximal pain levels from the day after the previous training session. Predefined cut-off points were applied; VAS ≤ 20 was considered “safe”, VAS ≤ 50 was considered “acceptable”, and VAS > 50 was considered “high risk” (26). The selection of pain score and the division of “safe”, “acceptable”, and “high risk” were based on other studies applying training to patients with hip osteoarthritis (13, 27). Acceptable adherence to training was a priori defined as an individual training attendance of ≥80% and drop-out was defined as a patient included in the study who for any reason fails to continue the training and complete the post-test. Adverse events were defined as musculoskeletal injury or cancelled sessions due to pain or other unexpected harmful events associated with the PRT intervention.
Descriptive measurements. Body height, weight and body mass index (BMI) were measured (Table I), the latter by a conventional bioimpedance leg-to-leg method, with a custom-built apparatus (Tanita-Body Composition Analyzer SC-330MA, Tanita Europe B.V., Amsterdam, The Netherlands).
Pre- and post-tests. Before the physical tests at both pre- and post-tests sessions, patients filled in The Copenhagen Hip and Groin Outcome Score (HAGOS). HAGOS is a valid, reliable and responsive PRO measure in young to middle-aged individuals with hip and groin pain (28).
The physical testing was initiated by a 5-min warm-up on a Monark ergometer cycle at a self-selected intensity. Shortly after the warm-up, patients performed 2 hop tests (single-leg standing distance jump (SDJ) (29) and single-leg countermovement jump (CMJ) (30)) and 4 muscle strength tests, for the hip flexors and the hip extensors. The tests were performed unilaterally on both sides. In all tests patients performed 2 submaximal trials (performed at intensities of 70% of maximal effort) followed by 3 maximal approved trials. However, if the patients increased their performance (> 10%) after the third attempt a fourth attempt was performed. The best trial for each leg in each test was used in the analysis and VAS scores were noted at the end of each test. Patients were randomized to start the tests with either their right or left leg, independent of which hip was scheduled for PAO. The hips were defined as the affected side (scheduled for PAO) and the non-affected side, the status of which was either: (i) healthy hip, (ii) diagnosed with HD but not symptomatic, (iii) diagnosed with HD with few symptoms, or (iv) previously operated with PAO.
The SDJ and CMJ were carried out as described previously by Reid et al. (29) and Larsen et al. (30), respectively. For SDJ the length of the hop was measured as the distance from the toe at the starting point to the heel at the landing position. CMJ was measured on a computerized system (Speedmat, Swift Performance Equipment, Queensland, Australia) connected to a contact mat that measured the flight time from which the flight height (in cm) was automatically calculated by the system software. Maximal voluntary contraction (MVC) was assessed using isokinetic dynamometry (Humac Norm, CSMI, Stoughton, MA, USA). The hip was positioned in 45° for isometric MVC and for isokinetic MVC the angular velocity was 60°/s. Torque was sampled at 1,000 Hz and stored for further analysis. The analyses were performed in a custom-made software (Labview – Multi Dynamic Analyzer). The method used is identical to that reported by Kierkegaard et al. (21).
Descriptive statistics are presented as means (standard deviation; SD), medians with range or as numbers with percentages. The distribution of data was initially assessed by histograms, residuals in scatterplots, kurtosis and skewness.
Changes from pre- to post-intervention were evaluated using paired t-tests provided that the assumption of normally distributed data was fulfilled. Wilcoxon signed-rank test was used in cases where data did not follow a normal distribution. If the results of parametric and non-parametric tests gave the same results, the results of parametric tests were presented. The level of significance was set at 5% (p ≤ 0.05). Stata 14.0 (Statacorp, Texas, TX, USA) and Excel 2013 were used for all statistical analysis. The purpose of this study was to test feasibility of a PRT programme; hence, power calculations for treatment effects were not performed.
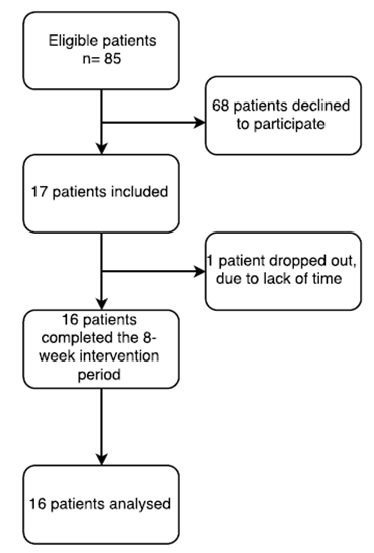
Of the 85 patients screened for eligibility, 17 (20%) were included and 16 completed the intervention (Fig. 1). One patient withdrew from the study during the first week due to lack of time to participate in the training sessions.
Fig. 1. Flow diagram of the inclusion process and final number of subjects available for analysis.
At baseline 75% of the included patients were women and 12 out of 16 patients were diagnosed with bilateral HD. Two patients had already undergone PAO for 1 hip and were scheduled for PAO on the other hip. One patient planned to undergo PAO for both hips within the next year (Table I).
Table I. Baseline characteristics of study participants (n = 16)
The mean (SD) adherence to the training sessions was 90.3% (9%). When related to the a priori adherence criteria 14 patients participated in 80% or more of the planned PRT training sessions, while 2 patients participated in only 75% of the planned sessions. Cancellations of sessions in these 2 patients were due to pain and a PAO surgery scheduled earlier than originally planned, respectively.
On average, a VAS ≤ 50 was reported during 95% of the completed sessions, while this was the case on 92.3% of the days following a training session (Fig. 2). Four patients cancelled training sessions due to pain (Table II). Two patients chose to postpone PAO after completion of the 8-week PRT programme, since they felt less pain in the hip and improved function and no longer felt the need for surgery.
No patients withdrew from the study due to pain or musculoskeletal injury. Two patients reported temporary pain of the knee joint after progressing to 10 RM and 1 patient experienced pain of the knee joint after the last training session (Table II).
Fig. 2. Percentage distribution of patients with pain scores of visual analogue scale (VAS) ≤ 20 (safe), VAS > 20–50 (acceptable) and VAS >50 (high risk). (A) Pain score during exercise. The pain score is the mean of all exercises and all training sessions within a 2 week period of the intervention. (B) Pain score the day after a training session. This score was reported at the following training session. VAS: visual analogue scale 100 mm (0–100). p < 0.01**.
Table II. Adverse events during the intervention period (n = 16)
Mean VAS scores for all exercises (Fig. 3A) showed a significant decline from the first week to the last (–7.0, 95% CI [–13.0, –3.0] p = 0.028). As seen in Fig. 3B mean VAS scores on the day after a training session did not change significantly from the first week to the last week (–7.0, 95% CI [–16.0, 1.0] p = 0.105). In general, patients reported higher VAS scores on the day after a training session and no significant changes were found between the first and the last week (–3.1, 95% CI [–9.7, 3.5] p = 0.352).
Fig. 3. Mean pain scores from each training session for all patients on a visual analogue scale (VAS) 100 mm, VAS (ranging from 0–100). (A) Mean pain scores of all exercises performed at each training session during the intervention period. (B) Pain scores the day after a training session during the intervention period. Error bars are 95% confidence intervals (95% CI).
Significant improvements after the intervention were seen in 4 out of 6 HAGOS subscales: Symptoms (mean 12.1 points, 95% CI [2.9, 21.2], p = 0.015), Pain (mean 9.5 points, [0.9, 18.1], p = 0.032), Sport/recreation (mean 12.5 points, [4.0, 21.0], p = 0.01) and QoL (mean 7.5 points, [1.7, 13.3], p = 0.022).
Individual scores from all HAGOS subscales are shown in Fig. 4.
Fig. 4. Pre- and post-test results of Hip and Groin Outcome Score (HAGOS) for each subscale. A score of 100 indicates no symptoms and 0 indicates extreme symptoms. ADL: activities of daily living; Sport/rec: sport and recreation; PA: participation in physical activity; QoL: quality of life. White dots are individual scores at pre-test and grey dots are individual scores at post-test. Black squares are group means with 95% confidence intervals (95% CI). *p ≤ 0.05; **p < 0.01.
Due to technical issues, only 11 patients were included in the CMJ analysis. One patient was not able to perform the SDJ and CMJ with the non-affected side at pre-test due to a previous PAO surgery, but completed all post-tests on both legs after the 8 weeks of PRT. One patient did not complete SDJ on the non-affected side at the post-test due to knee pain. Due to severe pain 1 patient was not able to complete the isokinetic MVC pre-tests on the affected side, but was able to complete the post-tests. All results for functional performance and muscle strength tests including VAS scores are shown in Table III.
Table III. Performance tests and maximal voluntary contraction pre- and post- the progressive resistance training (PRT) intervention
The main finding of the present feasibility study was that 8 weeks of PRT was feasible in the included group of HD patients scheduled for PAO. In general, adherence to training was high, there were no drop-outs due to pain or adverse events. The majority of patients reported acceptable pain levels (VAS ≤50) during exercise and on the day after a training session throughout the intervention. Of note, pain scores during exercise decreased significantly from the first week to the last week of the PRT intervention. These results are in line with previous feasibility studies investigating PRT in patients with hip OA (13) and chronic hip pain (31).
An exercise adherence of 90.3% was found in this study, which is in line with other studies in related conditions reporting 93% and 89%, respectively (13, 31). Herman et al. (13) found that patients with hip OA reported acceptable pain scores (VAS ≤ 50) in 83% of all sessions (within training days and on the day after a training session) during preoperative progressive explosive resistance training. In our study, the level of reported acceptable pain was 95% during exercise and 92.3% on the day after a training session. There was a high number (37.5%) of VAS reports > 50 on the day after a training session during the first week of the intervention, but there was only one occasion (6.3%) of VAS reports > 50 during the last week of the PRT intervention. This indicates training adaptions to the PRT intervention, even though there was no significant decrease in pain the day after a training session from the first to the last week. Only 17 patients of the 85 eligible patients (~20%) were included in the present study, which is a rather low inclusion rate. Patients often declined to participate due to lack of time and difficulties in implementing a training programme into their life. The majority of patients with HD who are scheduled for PAO are young women who often have small children, which may explain the low inclusion rate in the current study. Other related studies have reported inclusion rates of 7.8–38.4 % (13, 15, 25, 31).
Four of the 6 HAGOS subscales showed significant improvements and, of these, the subscales “symptoms” and “sport/recreation” showed a change within the defined minimal important change (MIC) of 10–15 points (28). This suggests that improvements are perceived by the patients despite the fact that surprisingly few significant improvements in hip muscle strength were found. Several reasons may explain the moderate improvements observed in the present study on muscle strength with PRT. First, due to pain levels in the “high-risk” zone patients were not able to follow the planned progression model completely, which may have compromised the effects of PRT in these patients. Secondly, the performance of the hip muscles may be impaired due to potential arthrogenic neuromuscular inhibition during exercise and MVC tests, which could influence the performance of the patient (32). Thirdly, the composition of the training protocol, with exercises focusing on the lower extremity muscles, may not activate and stimulate the hip joint muscles sufficiently. Exercises such as hip abduction and adduction were not included in the training protocol, which should be considered in future trials. Hip extensor muscles were used in leg press and lunges, but more specific exercises targeting hip extension could be beneficial for the hip joint, as suggested by Freeman et al. (32). Unfortunately, the lack of studies of good quality including patients with HD makes comparisons of the present results difficult. However, HD may predispose to development of secondary hip OA, making studies assessing the effect of exercise in patients with hip OA a relevant comparator. A systematic review of Pelland et al. (33) assessed 21 studies evaluating the effects of resistance training (RT) on adults with OA and reported beneficial effects of RT on strength, pain, function and quality of life (33). Several studies investigating muscle strength in patients with hip OA and hip groin pain have included training protocols focusing on hip flexion and extension, hip abduction and adduction. Importantly, improvements in muscle strength, leg extension power and return to sport were reported when including these exercises during interventions (13, 14, 34, 35). Accordingly, it has been demonstrated previously that patients with HD show deficits of the hip flexors (23), which is why this exercise was included in the present PRT programme. Since only hip flexion was a specific hip joint exercise and only MVC tests of isometric HF and isokinetic concentric HF showed significant improvements, it seems that only a restricted exercise stimulus is needed to induce general strength improvements of the hip. Although few significant muscle strength improvements were found in the present study, the mean decreased level of pain during MVC tests on the affected side showed a change within the suggested MIC of 15.0–20.0 mm (36, 37). The decrease in pain during maximal tests suggests that pain during high muscle performance tasks can be reduced by PRT in patients with HD.
A major limitation of the present study is the lack of a control group and the small sample size, which results in low statistical power when trying to detect changes. Only 20% of the eligible patients were included in this study and only 4 of those were men, which somewhat negatively affects the external validity. However, the few men included in the study simply reflects the male/female distribution in patients scheduled for PAO (38). Furthermore, VAS scores for each patient were not registered before each training session, making it difficult to determine whether exercise-related pain measured the day after a training session was related to the exercise or just reflected the patients’ normal level of pain. In addition, pain scores on the day after a training session could be subject to recall bias, since the score was first collected at the next training session.
To our knowledge, a PRT intervention has not been described previously in patients with symptomatic HD. Muscle-tendon-related pain exists in approximately half of patients with HD scheduled for PAO (39). These patients have a high prevalence of muscle-tendon-related pain in the iliopsoas and the hip abductors, and the pain is negatively associated with hip disability and muscle strength. The high prevalence and muscle-tendon-related pain in the hip flexors and abductors imply that clinicians have to re-evaluate the cause of pain from HD as solely being derived from the hip joint, and address the muscle-tendon-related pain when planning conservative or surgical treatment in patients with HD. The PRT applied in this study addresses the muscle-related pain and the reduced muscle strength, and it has the potential to be a future conservative treatment modality for patients with symptomatic HD. The natural history of HD is poorly understood and training may accelerate development of OA; however, this has not yet been studied. Information that regular physical exercise can decrease pain in the hip joint, improve symptoms and quality of life is important when informing patients with HD about potential treatment options. Moreover, many patients are reluctant to exercise due to fear of increased joint pain.
This study provides information that a higher level of pain should be expected in the initial period of a PRT exercise intervention, followed by a decrease in pain level with more training sessions completed and a higher degree of pain the day after a training session than during the exercises. In conclusion, 8 weeks of PRT is feasible for patients with HD, based on the recorded adherence, few adverse events, no drop-outs due to pain, and decreased or unchanged pain levels during exercise and on the day after training. The study further indicates potential improvements in HAGOS subscales, functional performance, pain scores and muscle strength after the PRT intervention, but this requires confirmation in a well-powered future RCT.
This study was supported by grants from Vanførefonden and Aase and Ejnar Danielsens Foundation.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize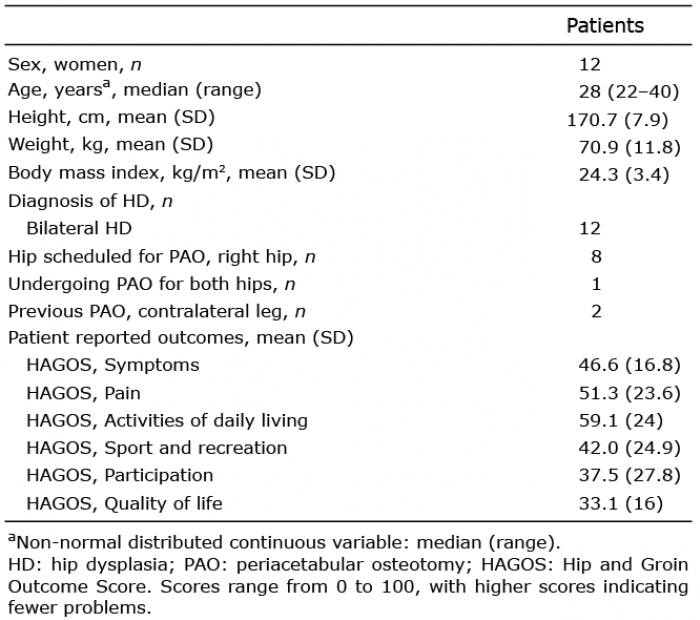 Click to show fullsize
Click to show fullsize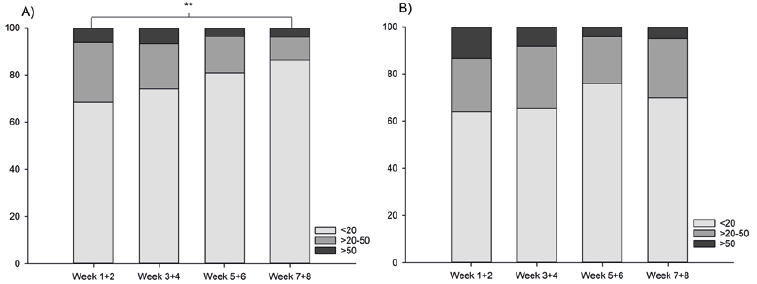 Click to show fullsize
Click to show fullsize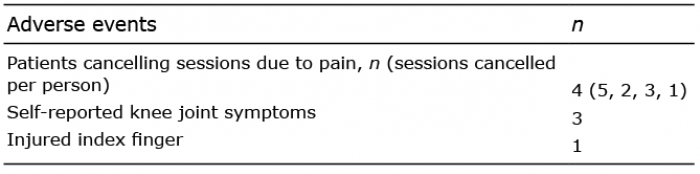 Click to show fullsize
Click to show fullsize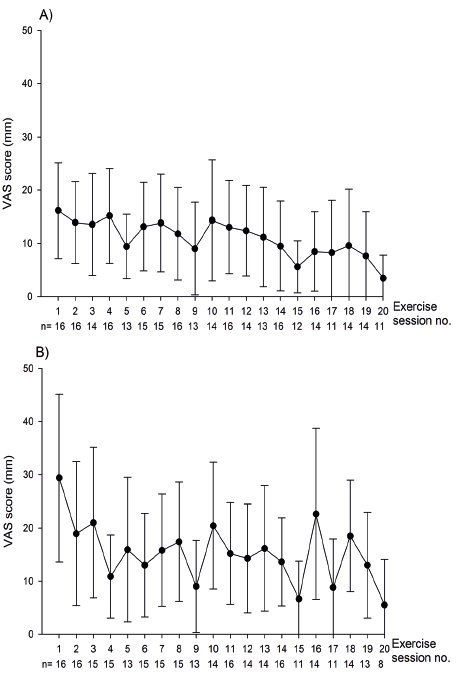 Click to show fullsize
Click to show fullsize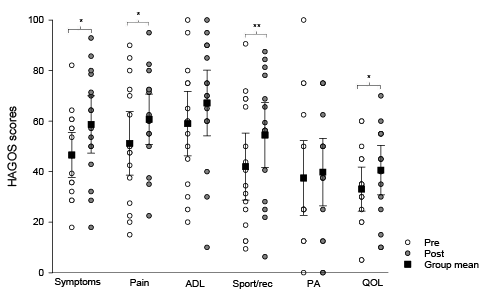 Click to show fullsize
Click to show fullsize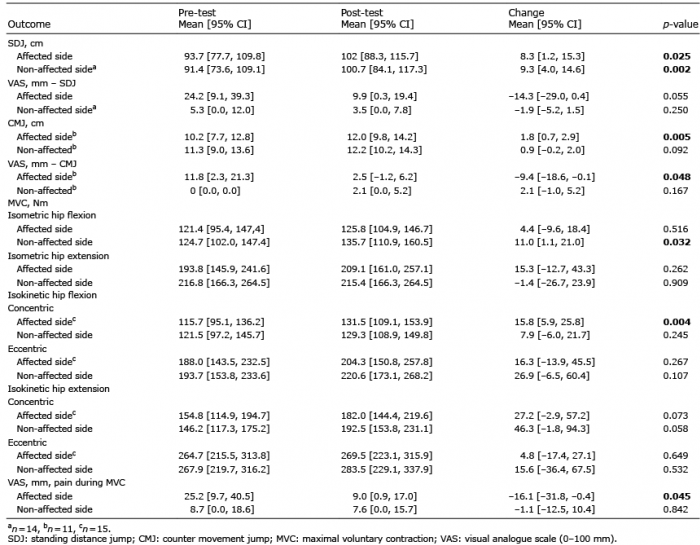 Click to show fullsize
Click to show fullsize